1 Policy summary
Safeguarding means protecting an adult’s right to live in safety, free from abuse and neglect. It is about people and organisations working together to prevent and stop both the risks and experience of abuse or neglect, while at the same time making sure that the adult’s wellbeing is promoted (Care Act, 2014). This includes where appropriate, regard for their views, wishes, feelings and beliefs. For people who are unable to protect themselves, additional measures should be provided to ensure their safety and wellbeing.
2 Introduction
Adult safeguarding can be complex and diverse and cover a wide range of activity from prevention through to multi-agency responses to stop harm. The adults should be central to the safeguarding process and their wellbeing must be promoted. Section 1 of the Care Act (2014) includes protection from abuse or neglect as part of the definition of well-being.
People can have complex lives and being safe is one of the things they want for themselves. We should work with the adult to establish what being safe means to them and how it can best be achieved. The trust is committed to ensuring the wellbeing of all adults through adherence, in all activity, to the six principles of adult safeguarding (Care Act, 2014):
- Empowerment: presumption of person led decisions and informed consent. Ensuring the service users wishes and their aspired outcomes are at the heart of any decision-making process.
- Protection: support and representation for those in greatest need.
- Prevention: it is better to act before harm occurs.
- Proportionality: proportionate and least intrusive response appropriate to the risk presented.
- Partnership: local solutions through services working with their communities. Communities have a part to play in preventing, detecting, and reporting neglect and abuse.
- Accountability: accountability and transparency in delivering safeguarding.
3 Purpose
This safeguarding adults policy aims to direct and support staff in the recognition, raising and managing of concerns of abuse and neglect of an adult at risk (person aged 18 years or older). This policy provides a clear framework to ensure that all staff are aware of their responsibilities and accountabilities, as identified by both legislation and locally established procedures, in relation to safeguarding adults at risk.
4 Scope
This policy is applicable to all trust staff, agency staff and other staff not employed directly by the trust such as volunteers who in the course of their duties, may come into contact directly with, or who may become party to information about, safeguarding adults’ issues.
5 Procedure
5.1 Quick guide
5.1.1 Concerned
You have a concern that an adult with care and support needs is at risk of, or is experiencing, abuse or neglect.
5.1.2 Safety
- Ensure the immediate safety and welfare of the adult at risk and any others who may be affected (including children).
- Consider if the emergency services are required.
5.1.3 Advice
- Seek advice from a safeguarding supervisor or the trust Safeguarding team.
- Advice is also available from the local authority safeguarding team both inside, and outside, of working hours.
5.1.4 Report
- Complete the safeguarding concern form.
- Complete an incident report.
5.1.5 Record
- Update the electronic patient record.
- Include actions taken to mitigate the risk.
5.2 Adult at risk
An “adult at risk” is defined by the Care Act (2014) as a person:
- who is 18 years and over
- who has needs for care and support (whether the local authority is meeting any of those needs)
- is experiencing, or at risk of, abuse or neglect
- who as a result of those care and support needs is unable to protect themselves from either the risk of or the experience of abuse or neglect
Care and support needs: The Care Act (2014) does not define what “care and support needs” mean but the Social Care Institute of Excellence (SCIE) (2022) provides useful guidance
Under the Care Act (2014), local authorities must arrange for an independent advocate to support an adult at risk if they have substantial difficulty in being involved in the safeguarding process and where there is no appropriate individual available to support and represent the person’s wishes.
Compliance with, and adherence to, this policy will ensure that Rotherham, Doncaster and South Humber NHS Foundation Trust (RDaSH) meets the contractual requirements of the Care Quality Commission (CQC) Health and Social Care Act (2008) (regulated activities) Regulations (2014) regulation 13, safeguarding service users from abuse and improper treatment.
Compliance with this policy will also provide assurance that the Trust adheres to NHS England: Safeguarding children, young people and adults in the NHS Safeguarding accountability and assurance framework (2022).
This will be achieved by the delivery of the following objectives:
- to identify lines of accountability
- to raise awareness of the types of abuse and neglect and referral procedures with all new members of staff during induction
- direct staff to named safeguarding professionals within the trust who can offer advice and supervision if requested
- direct staff towards external sources of advice and local safeguarding procedures
5.3 Categories of abuse and neglect
Defining abuse or neglect is complex and rests on many factors. The term “abuse” can be subject to wide interpretation. It may be physical, verbal or psychological, it may be an act of neglect, or occur where a vulnerable person is persuaded to enter into a financial or sexual transaction to which they have not, or cannot, consent.
Abuse or neglect may be the result of deliberate intent, negligence, or ignorance. Exploitation can be a common theme in the experience of abuse or neglect. Whilst it is acknowledged that abuse or neglect can take different forms, the Care Act guidance identifies the following types of abuse or neglect.
| Category of abuse and neglect | Definition |
|---|---|
| Physical abuse | Including inappropriate or careless handling, hitting, slapping, pushing, kicking, misuse of medication, or inappropriate sanctions, unwarranted enforced isolation, or captivity. |
| Psychological abuse | Including emotional abuse, threats of harm or abandonment, deprivation of contact, humiliation, blaming, controlling, intimidation, coercion, harassment, verbal abuse, cyberbullying, isolation or unreasonable and unjustified withdrawal of services or supportive networks. |
| Sexual abuse | Including rape, indecent exposure, sexual assault, sexual acts, sexual harassment, inappropriate looking or touching, sexual teasing or innuendo, sexual photography, subjection to pornography or witnessing sexual acts to which the adult has not consented or was pressured into consenting. It also includes sexual exploitation which is exploitative situations, contexts and relationships where the person receives “something” (for example, food, accommodation, drugs, alcohol, mobile phones, cigarettes, gifts, money) or perceived friendship or relationship as a result of them performing, and another or others performing sexual acts. |
| Financial or material abuse | Including theft, fraud, internet scamming, exploitation, coercion in relation to an adult’s financial affairs or arrangements, including in connection with wills, property, inheritance or financial transactions, or the misuse or misappropriation of property, possessions, or benefits. |
| Neglect or acts of omission | Includes ignoring medical or physical needs, failure to provide access to appropriate health, social care or educational services, the withholding of the necessities of life, such as medication, adequate nutrition and heating, hygiene, privacy, and dignity. |
| Self-neglect | Includes a person neglecting to care for their personal hygiene, health, or surroundings; or an inability to provide essential food, clothing, shelter or medical care necessary to maintain their physical and mental health, emotional wellbeing and general safety. It includes behaviour such as hoarding. Each local authority has a procedure to follow, see below: |
| Discriminatory | Including forms of harassment, bullying, slurs, isolation, neglect, denial of access to services or similar treatment; because of race, gender and gender identity, age, disability, religion or because someone is lesbian, gay, bisexual, or transgender. This includes racism, sexism, ageism, homophobia or any other form of hate incident or crime. |
| Organisational abuse | Including neglect and poor care practice within an institution or specific care setting such as a hospital or care home, for example, or in relation to care provided in a person’s own home. This may range from one off incidents to ongoing ill treatment. It can be through neglect or poor professional practice as a result of the structure, policies, processes, and practices within an organisation. |
| Domestic abuse | Including an incident or a pattern of incidents of controlling, coercive or threatening behaviour, violence, or abuse, by someone who is, or has been, an intimate partner or family member regardless of gender or sexual orientation. This includes psychological or emotional, physical, sexual, financial abuse; so-called honour based violence, forced marriage or female genital mutilation (FGM). Link to the domestic abuse policy. |
| Modern slavery | Encompasses slavery, human trafficking, forced labour and domestic servitude. Traffickers and slave masters use whatever means they have at their disposal to coerce, deceive, and force individuals into a life of abuse, servitude and inhumane treatment. |
5.4 Abuse related issues
5.4.1 Sexual incidents
Any behaviour of a sexual nature that is unwanted, or makes another person feel uncomfortable or afraid. Sexual incidents can involve patients, colleagues, visitors, contractors, and volunteers either as a victim or a perpetrator. This policy is in relation to patients, see the sexual misconduct policy for incidents relating to any others. Sexual incidents can be broadly defined as physical or non-physical:
5.4.1.1 Physical
- Rape.
- Attempted rape.
- Inappropriate touching anywhere (including use of objects).
- Non-consensual masturbation of either or both persons.
- Non-consensual sexual penetration or attempted penetration of vagina, anus or mouth with objects other than penis.
- Non-fatal sexual strangulation or suffocating.
5.4.1.2 Non-physical: sexual harassment
- Inappropriate looking.
- Sexual teasing or innuendo.
- Sexual harassment.
- Unwanted exposure of pornography.
- Witnessing sexual acts.
- Indecent exposure.
| Term | Definition |
|---|---|
| Grooming | Is when a person builds a relationship with a child, young person or an adult so they can abuse them and manipulate them into doing things sexual, financial or other illegal acts. It can take place online or in person and can happen over a short or long period of time. |
| Sexual safety | Feeling safe from any unwanted behaviour of a sexual nature and feeling safe from sexual harm. |
| Sexual consent | Consent is defined by section 74 Sexual Offences Act (2003) as “Someone consents to vaginal, anal or oral penetration only if she or he agrees by choice to that penetration and has the freedom and capacity to make that choice”. |
5.4.1.3 Process to follow if an adult makes an allegation of a sexual incident
If rape or attempted rape or non-consensual penetration of vagina, anus or mouth and, or non-fatal strangulation:
- report immediately to the police (999) and escalate to line manager and safeguarding team
- preserve any evidence, for example, bag, clothing and, or bedding to prevent cross contamination (police will need this for forensic examination)
- try to prevent individual from washing
- if the individual requires medical treatment, then this must be prioritised, and history of injury relayed to medical team or the emergency department to ensure preservation of evidence
- provide individual privacy and support while waiting for the police
- if the alleged perpetrator is a patient, then provide support until police arrive
- if the alleged perpetrator is a colleague, then police will lead investigation until trust policies can be invoked
- if alleged perpetrator leaves the incident area, obtain a description, do not put yourself at risk to pursue
- if a sexual incident has occurred to contact 999 or 101 depending on severity
- immediate action should be taken to protect the individual from further harm
- if the individual is an “adult at risk” as defined by the Care Act (2014) then a safeguarding concern must be submitted to the local authority, see section 5.5
- if the individual is a child (under the age of 18) please refer to the safeguarding-children-policy
- an incident report must be completed for any sexual incident (please refer to incident management policy) and if this involves a patient, document the incident and what actions were taken on the electronic record (please refer to healthcare record keeping policy)
- all incidents must be reported to Safeguarding team and if out of hours to on call manager
- if the alleged perpetrator of a sexual incident is a colleague, then the procedure for managing allegations against people in positions of trust (PiPoT) will be invoked
Consideration must be made for patients who may not have capacity to make decisions for themselves for example patients with learning disabilities and patients detained under the Mental Health Act. For advice and support please contact trust Mental Capacity Act lead or the safeguarding team.
5.4.1.4 Other considerations
Further to the above consideration must be made in conjunction with the police and Consultant whether the victim requires:
- emergency contraception and follow-up pregnancy test
- post exposure prophylaxis (PEP) for human immunodeficiency virus (HIV)
- referral to sexual abuse referral centres (SARC)
5.4.1.5 Non-physical incidents: sexual harassment
Sexual Harassment is unlawful and prohibited under the Equality Act (2010). The term sexual harassment encompasses a wide range of behaviour, which may take place in person, online or over the phone. A single event or a series of events can amount to sexual harassment. This can be aimed at an individual or there may be a culture of sexual harassment which is not specifically aimed at one person.
Any such behaviours should be reported via incident report and escalated to line manager. Some people may feel more comfortable to reporting via safeguarding team and, or Freedom to Speak Up (FTSU).
5.4.1.6 Impact of sexual harassment
The negative impact on people who have been victims of this behaviour can be presented in different ways and we should be mindful of this. Some symptoms are:
- post traumatic stress disorder
- anger
- guilt self blame
- lack of trust especially if professional boundaries have been breached
5.4.1.7 Reducing the risk and keeping safe
- Be vigilant and take action if any observations are made regarding sexual incidents.
- Single gender corridors and bathrooms.
- Identify risks and support with the devising of protection plans.
- Ensure that any historical abuse is documented, and care plans devised.
- Colleagues will listen and respond to any sexual incidents.
- Colleagues will be trained on managing professional boundaries and maintaining professional standards.
- Utilise Oxevision and closed-circuit television (CCTV).
- Seek advice and support from the safeguarding team and, or patient safety team.
5.4.1.8 Colleague as perpetrator
- Report to police.
- Instigate person in a position of trust (PiPoT) procedures if the victim is an adult.
- Instigate local authority designated officer (LADO) procedures, if it is a child or if the perpetrator works with children.
- Utilise the sexual misconduct policy.
- Sign post to Respect phone line.
- Refer to Health and Wellbeing team.
- Ensure that the victim and alleged perpetrator do not have any contact.
5.4.1.9 Patient as a victim and as a perpetrator
If any incidents of a sexual nature take place on inpatient wards between patients, this is a safeguarding incident regardless of consent or capacity at the time. Decisions made by someone who is unwell, lacks capacity and vulnerable, can impact not only on their lives but family too. As a trust we have a duty to ensure their safety and to put measures in place to minimise the risk. This would include putting immediate safeguards in place, discussions with the individuals involved and capacity assessment regarding decision-making. Support can be sought from the safeguarding team, Mental Capacity Act lead and the Patient Safety team.
5.4.2 The movement in and out of locality for children and vulnerable adults where there are safeguarding concerns
Learning from both adult and child safeguarding reviews have recognised that in cases where children or vulnerable adults have relocated and there are safeguarding concerns this can lead to significant harm or death. A common theme is ineffective communication and information sharing where safeguarding concerns are suspected or known.
Practitioners should be proactive in sharing information where children/vulnerable adults are at risk of harm or abuse. The law does not prevent the sharing of sensitive, personal information between organisations where there is a safeguarding concern (Working together to safeguard children 2023) (Care Act 2014).
Where a child or vulnerable adult is known to have moved to a different locality and safeguarding concern are suspected or known, the following actions should be taken prior to any discharge:
- verbal and written liaison with receiving service providers for example GP, Health Visitor, School nursing, and Mental health services.
- consider threshold document, is a safeguarding referral required to the receiving local authority.
- if you suspect a child or vulnerable adult is in immediate danger, please contact 999
5.4.2.1 Where a child or vulnerable adult whereabouts are unknown (missing) and there are known or suspected safeguarding concerns
The definition of missing from Royal college of policing (2016) is anyone whose whereabouts cannot be established will be considered as missing until located, and their well-being or otherwise confirmed.
Practitioners should use professional curiosity to consider the family dynamic, family history, social vulnerabilities, safeguarding history, attendance or engagement with professionals and any other factors that may increase vulnerability or risk. If safeguarding concerns are identified and a child or vulnerable adult is considered missing the following actions should be taken:
- make enquiries with GP, other professionals or agencies likely to be involved, for example, health professionals, education, employment, housing, child health, probation or youth justice system to establish if they know of their whereabouts
- contact local authority safeguarding team or MASH to report concerns of missing child or vulnerable adult.
- report concerns of missing child or vulnerable adult to police.
- complete a trust incident report
- document any actions taken in electronic patient record
5.4.2.2 Notification of missing families to the trust
When a national notification of a missing family is received into the trust Safeguarding team and they are currently open to a trust service, the safeguarding team will inform the manager of the service for information sharing or action.
The safeguarding team will respond to the alerting authority advising that the family are known to trust services. The contact details of the trust service will be shared with the alerting authority for the purposes of information sharing.
5.4.3 Pressure ulcers
Most pressure ulcers are entirely preventable through risk assessment and the implementation of pressure relieving measures. The simple fact that a person at risk has a pressure ulcer, even a category 3 or category 4, or multiple pressure ulcers, more than 3 or 4 at a lower category or mixed categories, is not in itself a reason to suspect abuse or neglect.
There are several factors to help decide whether it potentially indicates neglect or whether it indicates a need for care providers to improve practice.
These factors include:
- the person’s physical health and existing medical conditions
- any skin conditions the person may have any other signs of neglect, such as poor personal hygiene
- the appropriateness of their care plan and whether it has been properly carried out
- the person’s own view, and the views of their family and friends, on the treatment and care
Staff will record in the appropriate document or care plan the patients or service users and carers understanding and comprehension of pressure ulcer prevention or management plans. This must include information on the patient’s capacity to understand the information to ensure informed decision-making. All safeguarding concerns must be reported. Link to the tissue viability and wound care manual.
5.4.4 Prevent
Prevent is part of the government counterterrorism strategy. One of the national objectives for prevent is to avert people from being drawn into terrorism and ensure that they are given appropriate advice and support. If you suspect someone, whether service user, staff or visitor is at risk of radicalisation you must report it. See prevent strategy for the process to follow.
5.4.5 Managing allegations against people in positions of trust (PiPoT)
This is when a person who is working with adults with care and support needs has:
- behaved in a way that has harmed or may have harmed an adult with care and support needs
- possibly committed a criminal offense against or related to an adult with care and support needs
- behaved towards an adult with care and support needs in a way that indicates she or he is unsuitable to work with such adults
- behaved in a way that has harmed children or may have harmed children which means their ability to provide a service to adults with care and support needs should be reviewed
- been subject to abuse themselves and there is evidence that this impacts on their suitability to work with adults with care and support needs
All allegations of abuse, neglect, or maltreatment of adults with care and support needs by a person in a position of trust must be taken seriously and treated in accordance with the managing allegations against people in positions of trust (PiPoT) procedure.
5.4.6 Raising concerns at work (whistleblowing)
Trust staff come into contact with lots of different agencies caring for vulnerable people on a daily basis. During a shift a member of staff could potentially witness a colleague or care provider abusing an adult considered to be at risk. Because abuse is a sensitive and difficult area it can be tempting not to take action when abuse is occurring within our work environment, especially when the abuser is a member of staff. However, ignoring our concerns can risk:
- reinforcing abusive behaviour and perhaps put others at risk
- no action, including support and protection, for all those in the situation
- further misery because distress is not acknowledged
- vulnerable victims seen as not needing or entitled to care, treatment, support or justice
- perpetuation of a criminal act by the perpetrator
The trust has a Freedom to Speak Up: raising concerns (whistleblowing) policy which sets out roles and responsibilities of staff and the processes involved.
5.4.7 Fabricated or induced illness
Adults can sometimes be presented to professionals by carers, as having physical or mental health problems when the adult has no recognised medical condition and the symptoms cannot be accounted for by any known illness. If these actions are causing, or putting an adult at risk, the situation may be referred to as fabricated or induced illness by carers’ (FII).
The Care Act (2014) does not mention FII and FII is not a specified form of adult abuse. The Care Act (2014) is clear that our responsibility to safeguard adults includes stopping harm and abuse, where possible or limiting the impact by preventing harm and abuse. The Royal College of Psychiatrists (2020) produced guidance for assessing and managing cases of fabricated or induced illness which can be found here: Fabricated or induced illness in adults.
5.5 Responding to adult safeguarding concerns
Make an immediate evaluation of the risk and take steps to ensure that the adult is in no immediate danger. Where appropriate, call 999 for emergency services if there is a medical emergency, other danger to life or risk of imminent injury, or if a crime is in progress.
Consider if there are other adults with care and support needs or children who are at risk of harm and take appropriate steps to safeguard them. The process for reporting safeguarding children concerns can be found in the safeguarding children manual.
Contact the trust Safeguarding team for advice if required.
Report the incident internally on the incident reporting system.
Ensure all decision-making is recorded in the electronic patient records, using the safeguarding adult template.
All adult safeguarding concerns must be reported to the Adult Safeguarding team in the local authority on the same day that the concerns were identified.
See below for contact details:
- North Lincolnshire safeguarding adult concern form or phone: 01724 297 000
- Rotherham safeguarding adult concern form or phone: 01709 822 330
- Doncaster safeguarding adult concern form or phone: 01302 737 063
5.5.1 Involving the adult
Making safeguarding personal (MSP) stresses the importance of keeping the adult at the centre. Under making safeguarding personal the adult is best placed to identify risks, provide details of its impact and whether they find the mitigation acceptable. Working with the adult to lead and manage the level of risk that they identify as acceptable creates a culture where:
- adults feel more in control
- adults are empowered and have ownership of the risk
- there is improved effectiveness and resilience in dealing with a situation
- there are better relationships with professionals
- good information sharing to manage risk, involving all the key stakeholders
- key elements of the person’s quality of life and wellbeing can be safeguarded
Using making safeguarding personal principles, the key focus is on developing a real understanding of what people wish to achieve, agreeing, negotiating and recording their desired outcomes, working out with them (and their representatives or advocates if they lack capacity) how best those outcomes might be realised and then seeing, at the end, the extent to which desired outcomes have been realised.
5.5.2 Record keeping
As soon as possible on the same day, make a written record of what has been seen, told or there are concerns about. Written records must be as accurate as possible and contain what was said and done by the people involved. This is important for defensible decision-making which means recording a clear rationale for all the decisions made and the discussions that led to the decision.
The written record will need to include:
- when you were told about or witnessed the incident
- who was involved
- exactly what happened or what you were told, using the persons own words
- the views and wishes of the adult
- the appearance and behaviour of the adult and, or the person making the disclosure
- any injuries observed
- any actions or decisions taken
- any previous incidents that have caused you a concern
All safeguarding incidents must be reported the incident reporting system. This includes all incidents of concern involving adults even if it has not resulted in a referral to social care. The incident form must be completed as soon after the incident has taken place or been identified as occurring, and no later than one working day afterwards. Any member of staff who is unable to complete the incident form for any reason within this time frame must inform their line manager.
5.5.3 Information sharing
Safeguarding enables the sharing of information without the persons consent if it is for the purpose of the detection and prevention of crime and also where safeguarding of children is required (HM Government, 2018).
5.5.3.1 Seven golden rules for information sharing
- Remember that the general data protection regulation (GDPR) is not a barrier to sharing information but provides a framework to ensure that personal information about living persons is shared appropriately.
- Be open and honest with the person (and, or their family where appropriate) from the outset about why, what, how and with whom information will, or could be, shared, and seek their agreement, unless it is unsafe or inappropriate to do so.
- Seek advice if you are in any doubt, without disclosing the identity of the person where possible.
- Share with consent where appropriate and, where possible, respect the wishes of those who do not consent to share confidential information. You may still share information without consent if, in your judgement, that lack of consent can be overridden in the public interest. You will need to base your judgement on the facts of the case.
- Consider safety and wellbeing: base your information-sharing decisions on considerations of the safety and wellbeing of the person and others who may be affected by their actions.
- Necessary, proportionate, relevant, accurate, timely and secure: ensure that the information you share is necessary for the purpose for which you are sharing it, is shared only with those people who need to have it, is accurate and up to date, is shared in a timely fashion, and is shared securely.
- Keep a record of your decision and the reasons for it – whether it is to share information or not. If you decide to share, then record what you have shared, with whom and for what purpose.
5.5.4 Capacity and consent
An adult’s legal right to consent marks the fundamental difference in approaches to adult safeguarding compared with children’s safeguarding arrangements. It is normally essential to seek the service users consent before any safeguarding process begins. However, there may be issues in regard to the service user’s mental capacity to consent. In this instance, refer to the Mental Capacity Act (2005) policy.
5.5.5 Reporting without consent
In cases where there is an overriding public interest or if gaining consent would put the adult at further risk then the concern must be reported. This includes situations where:
- there is a serious risk of harm to the wellbeing and safety of the adult or a risk of harm to others
- other adults or children could be at risk from the person causing harm
- it is necessary to prevent crime or if a crime may have been committed
- the person lacks the capacity to consent
If a staff member is unsure whether to report the advice can be sought from the trust Safeguarding team email rdash.safeguardingadults@nhs.net or the Adult Safeguarding team in the local authority:
- North Lincolnshire: 01724 297 000
- Rotherham: 01709 822 330
- Doncaster: 01302 737 063
5.6 Advocacy services
Advocacy promotes equality, social justice, and social inclusion. It can empower people to speak up for themselves. Advocacy can help people become more aware of their own rights, to exercise those rights and be involved in and influence decisions that are being made about their future. In some situations, an advocate may need to represent another person’s interests. This is called non-instructed advocacy and is used when a person is unable to communicate their views.
5.6.1 Advocacy services North Lincolnshire: People of Here Want Equal Rights (POhWER)
- Phone: 0300 456 2370
- Email: pohwer@pohwer.net
Independent advocacy for:
- NHS complaints advocacy
- independent mental health advocacy
- independent mental capacity advocacy including deprivation of liberty safeguards (DoLS)
- relevant person’s paid representative services (RPPR)
- care act advocacy
- generic non-statutory advocacy: for residents of North Lincolnshire or those registered with a GP in the area.
5.6.2 Advocacy services Rotherham: Absolute advocacy
Unit 3
Bessemer Way
Bessemer Business Park
Rotherham
S60 1EN
- Phone: 01709 794 294
- Email: enquiries@absoluteadvocacy.org.uk
- Absolute advocacy
Independent advocacy for:
- people with mental health needs
- older people
- people with physical or sensory impairment
- Care Act advocacy
- independent mental capacity advocate (IMCA)
- deprivation of liberty safeguards (DoLS) advocate
- independent mental health advocate (IMHA)
For a referral form please see Cloverleaf referral form.
5.6.3 Advocacy services Doncaster: Cloverleaf advocacy
Fourth Floor
Empire House
Wakefield Old Road
Dewsbury
WF12 8DJ
- Cloverleaf
- Phone: 01924 454 875
- Text number for referrals: 07860 021 502
- Email: referrals@cloverleaf-advocacy.co.uk
Independent advocacy for:
- community advocacy
- care and support advocacy
- care act advocacy
- independent mental capacity advocate (IMCA)
- deprivation of liberty safeguards (DoLS) advocate
- relevant person’s representative (RPR)
- independent mental health advocate (IMHA)
- NHS complaints advocacy
- children and young people’s advocacy
5.7 Section 42 enquiries
A section 42 enquiry relates to the duty of the local authority to make enquiries, or have others do so, if an adult may be at risk of abuse or neglect. This happens whether the authority is providing any care and support services to that adult. It aims to decide what, if any, action is needed to help and protect the adult.
The scale of the enquiry, who leads it, the format it takes and how long, will depend on the particular circumstances.
It will usually start with asking the adult about their view and wishes, which will often determine what next steps to take.
Everyone involved in an enquiry must focus on improving the adult’s wellbeing and work together to that shared aim. At this stage, the local authority also has a duty to consider whether the adult requires an independent advocate to represent and support the adult in the enquiry.
The objectives of an enquiry into abuse or neglect are to:
- establish facts
- ascertain the adult’s views and wishes
- assess the needs of the adult for protection or support and redress, and how they might be met
- protect the person from the abuse and neglect, in accordance with the wishes of the adult
- make decisions about what follow-up action should be taken with the person or organisation responsible for the abuse or neglect
- enable the adult to achieve resolution and recovery
An enquiry could range from a conversation with the adult, or their representative or advocate, prior to initiating a formal enquiry under section 42, right through to a much more formal multiagency plan or course of action.
What happens as a result of the enquiry should reflect the adult’s wishes wherever possible, as stated by them or by their representative or advocate.
If the adult lacks capacity to engage with the process, any decision made must be in their best interests and be a proportionate response to the concern
The local safeguarding adults procedures can be found below:
- North Lincolnshire safeguarding adults policy and procedure
- Rotherham safeguarding principles and the approach for South Yorkshire
- Doncaster safeguarding adults procedure
5.8 Adult safeguarding and the Human Rights Act (1998)
In respect of safeguarding adults at risk, there are 4 articles that are of relevance:
- article 2, protect the right to life. This means public authorities must sometimes take positive steps to protect people if their lives are in danger
- article 3, affords freedom from degrading and inhumane treatment. Article 3 is breached when public bodies carry out or are responsible for abusive care and treatment; that is allowing or ignoring actions when they should not have done so. There is a positive duty under Article 3, for a public body to intervene when abuse is performed by one private individual against another
- article 5, enshrines the right to liberty and security. People who lack mental capacity are one of the categories when people can be deprived of their liberty. Legal procedures are set out in the Mental Capacity Act (2005) and the Mental Health Act (1983) and should be followed. If they are not adhered to, it may lead to a breach of article 5. A deprivation of liberty under the Mental Capacity Act describes a best interest decision made regarding a person who lacks mental capacity to decide about care, treatment or living arrangements. Such deprivations must be legally authorised under the provisions of the Mental Capacity Act or by order of the court of protection
- article 8, guarantees the right to a private life, family life and a home life. Public bodies can interfere with people’s right to respect for private and family life, home and correspondence but they must be able to show that such action is lawful, necessary and proportionate in order to protect national security, public safety, the economy, health or morals, prevent disorder or crime or protect the rights and freedoms of other people
All safeguarding interventions need to consider and respect the above articles.
6 Training implications
6.1 Safeguarding adults manual 1
- Employee groups requiring training: staff required to be competent with level 1 safeguarding adult training.
- Frequency: every 3 years.
- Length of training: 2 hours.
- Delivery method: e-learning.
- Training delivered by: e-learning for healthcare.
- Where are the records of attendance held: electronic staff record (ESR).
6.2 Safeguarding adults manual 2
- Employee groups requiring training: staff required to be competent with level 2 safeguarding adult training.
- Frequency: every 3 years.
- Length of training: 3 hours.
- Delivery method: e-learning.
- Training delivered by: e-learning for healthcare.
- Where are the records of attendance held: electronic staff record (ESR).
6.3 Safeguarding adults manual 3
- Employee groups requiring training: staff required to be competent with level 3 safeguarding adult training.
- Frequency: annually.
- Length of training: 3 hours.
- Delivery method: multiple.
- Training delivered by: blended learning.
- Where are the records of attendance held: electronic staff record (ESR).
Trust safeguarding training intranet page (staff access only).
7 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
7.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
Consequently, the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity, and respect, (when appropriate this should also include how same sex accommodation is provided).
7.1.1 Indicate how this will be met
No issues have been identified in relation to this policy.
7.2 Mental Capacity Act
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individual’s capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individuals’ informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all colleagues working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason, all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005)to ensure that the rights of individual are protected, and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
7.2.1 Indicate how this will be achieved
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005).
8 Links to any other associated documents
- Domestic abuse policy
- Freedom to speak up: Raising concerns (whistleblowing) policy
- Healthcare record keeping policy
- Incident management policy
- Information governance staff code of conduct
- Managing allegations against people in positions of trust (PiPoT) procedure
- Mandatory and statutory training policy
- Mental Capacity Act (2005) policy
- Prevent strategy
- Safeguarding children policy
9 References
- HM Government (1983) Mental Health Act
- HM Government (1998) Human Rights Act
- HM Government (2005) Mental Capacity Act
- HM Government (2008) Health and Social Care Act
- HM Government (2014) The Care Act
- HM Government (2018) Information Sharing. Advice for practitioners providing safeguarding services to children, young people, parents, and carers
- NHSE (2022) Safeguarding children, young people and adults in the NHS. Safeguarding accountability and assurance framework
- Royal College of Psychiatrists (2020) Assessment and management of adults and children in cases of fabricated or induced illness (FII)
- Social Care Institute of Excellence (2022) Practice examples: assessment and eligibility for the Care Act 2014
10 Appendices
10.1 Appendix A Reporting a child safeguarding concern
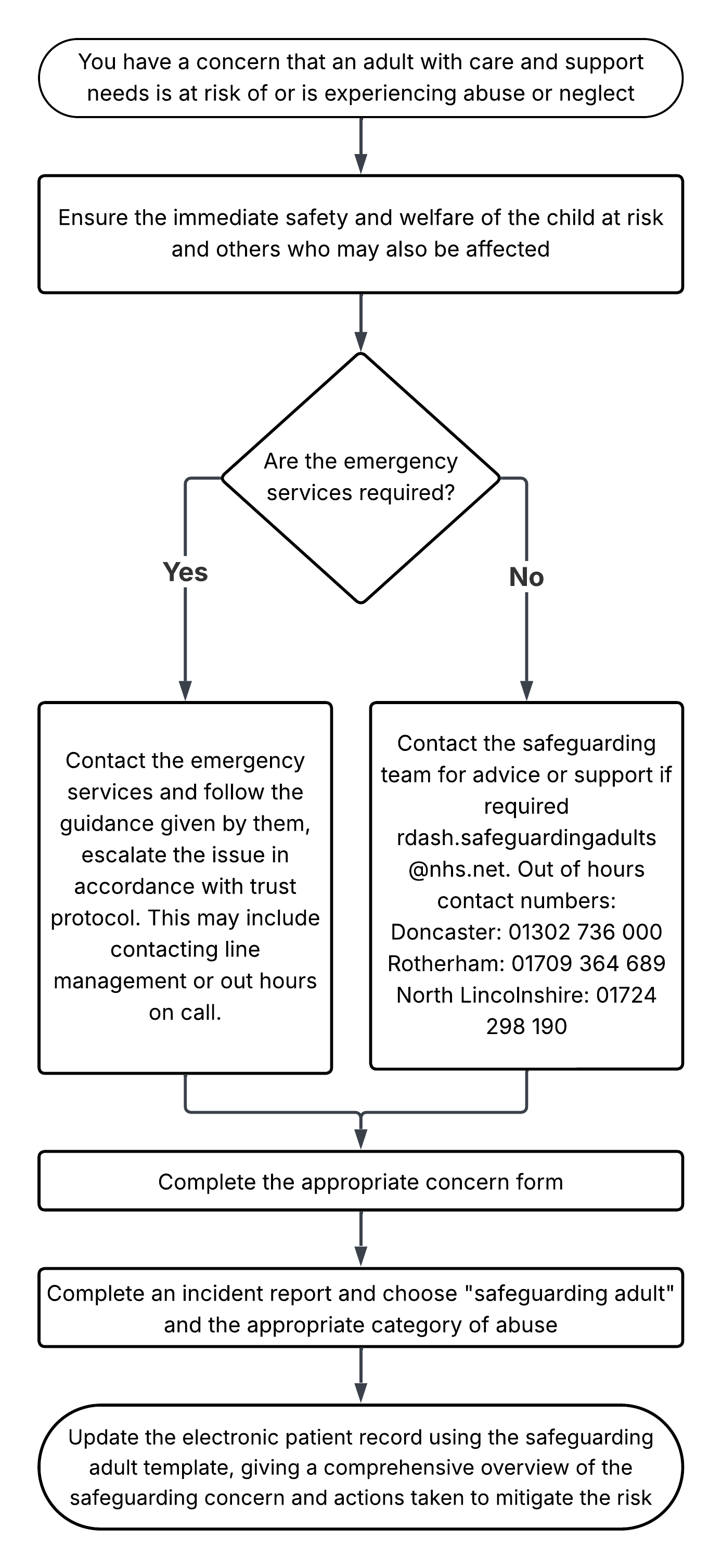
- You have a concern that an adult with care and support needs is at risk of or is experiencing abuse or neglect.
- Ensure the immediate safety and welfare of the child at risk and others who may also be affected.
- Are the emergency services required?
- Yes, contact the emergency services and follow the guidance given by them, escalate the issue in accordance with trust protocol. This may include contacting line management or out hours on call.
- No, contact the safeguarding team for advice or support if required rdash.safeguardingadults@nhs.net. Out of hours contact numbers:
- Doncaster: 01302 736 000
- Rotherham: 01709 364 689
- North Lincolnshire: 01724 298 190
- Complete the appropriate concern form:
- Complete an incident report and choose “safeguarding adult” and the appropriate category of abuse.
- Update the electronic patient record using the safeguarding adult template, giving a comprehensive overview of the safeguarding concern and actions taken to mitigate the risk.
10.2 Appendix B Responsibilities, accountabilities and duties
10.2.1 The trust
The chief executive and directors of the trust are responsible for ensuring that robust systems are in place to identify and manage the risks associated with safeguarding adult at risk and to support the effective multiagency partnership working and responses which are required.
This includes the identification and training of suitable staff to fulfil the roles set out within the multiagency safeguarding adult’s procedures. All staff are responsible for fulfilling their responsibilities to safeguard adult at risk.
10.2.2 The trust’s nominated executive director
The trust has a nominated executive director for safeguarding adults, who takes a professional lead in promoting best practice in safeguarding adults at board level. In this trust, the nominated executive director for safeguarding adults is the director of nursing and allied health professionals.
10.2.3 Deputy director of nursing (operational lead)
Has responsibility to provide expert advice, strategic and operational leadership for safeguarding and professional standards. To continually develop a proactive approach to safeguarding through collaboration with the local authority and other agencies. To ensure all mandatory and statutory requirements around safeguarding are met and develop support systems.
10.2.4 Nurse consultant safeguarding
Has responsibility to provide expert advice, strategic and operational leadership for safeguarding and professional standards. To continually develop a proactive approach to safeguarding through collaboration with the local authority and other agencies. To ensure all mandatory and statutory requirements around safeguarding are met and develop support systems.
10.2.5 Lead professional’s for safeguarding adults, named nurses or named professionals (practice leads)
Have responsibility to provide an expert professional leadership role in relation to safeguarding adults. To work at a strategic level across the health and the social care community, fostering and facilitating multiagency working and training in respect of safeguarding adults. To act as an expert resource on safeguarding adults issues, providing accessible, accurate and relevant information to staff.
The practice leads are responsible for delivering support, advice and guidance to the safeguarding managers and enquirers.
They have a key role in promoting best practice and are available as a source of advice or guidance and support for managers and staff involved in safeguarding.
10.2.6 Service managers, modern matrons or area clinical managers
Service managers, modern matrons or area clinical managers are responsible for:
- ensuring all staff have access to the relevant multiagency safeguarding adults procedures in their workplace
- maintaining compliance with the policy and multiagency safeguarding adults procedures within their services
- arranging staff attendance at training, updates in relation to safeguarding adults
- providing support for staff involved in safeguarding adults
10.2.7 Employees of the Rotherham, Doncaster and South Humber NHS Foundation Trust
Safeguarding is everybody’s business.
All employees (including volunteers) have a responsibility to safeguard and promote the wellbeing of adults at risk of harm. Employees must be able to recognise and report safeguarding concerns to their line manager or the Safeguarding team to ensure actions can be taken to address the concerns.
10.2.8 Safeguarding managers
Safeguarding managers are identified trust staff who have undertaken the multiagency safeguarding adults’ procedures and are responsible for:
- initiating preliminary fact finds
- overseeing the enquiry and supporting the enquirer
- arranging and chairing planning meetings, including the agreement of responsibilities, actions and timescales
- responsible for maintaining records and completion of appropriate documentation
- responsible for referring the adult at risk for advocacy (independent mental capacity advocate, independent care act advocate and independent domestic violence advocate)
- if the allegation is regarding a person in position of trust (PiPoT) to liaise with the Safeguarding team
- prepare interim protection plans
10.2.9 Safeguarding enquirers
Safeguarding enquirers are identified trust staff who have undertaken the multiagency training on conducting an enquiry. They are responsible for:
- coordinating the collation of information regarding the alleged abuse
- meeting with the adult at risk to identify what their outcomes for the enquiry are
- working with partner agencies if required
- liaising with the police if criminal activity
- liaise with safeguarding manager
- complete documentation
- ascertain on the balance of probability if abuse has taken place
- oversee the development of a risk management and protection plan
10.3 Appendix C Monitoring arrangements
10.3.1 Adherence to policy and process
- How and who by: training and supervision monitoring process.
- Reported to: safeguarding assurance group.
- Frequency: quarterly.
10.3.2 Adherence to policy and process
- How and who by: audit.
- Reported to: safeguarding assurance group.
- Frequency: annually.
Document control
- Version: 2.3.
- Unique reference number: 510.
- Approved by: clinical effectiveness meeting
- Date approved: 7 October 2025.
- Name of originator or author: nurse consultant for safeguarding.
- Name of responsible individual: chief nursing officer.
- Date issued: 30 October 2025.
- Review date: 30 April 2026.
- Target audience: all staff within the trust.
Page last reviewed: January 29, 2026
Next review due: January 29, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem